Facet blocks
A facet block is a semi-invasive procedure performed under fluoroscopic guidance . Unfortunately, the term "facet block" is generally used for two completely different techniques: a) the block of the 2 nerves innervating the facet joint (medial branch block), b) the intra-articular injection of the facet .
Indications:
-
Diagnosis : Facet blocks performed correctly have a very localized effect (virtually no effect on adjacent segments and no or very little systemic effect). This spatial specificity makes it possible to test the presumed origin of the pain. This is particularly useful in multisegmental disorders as is frequently the case with the cervical spine.
-
Therapeutic : In some situations, intra-articular facet blocks have a therapeutic effect. For example, it can allow a yellow ligament cyst to empty, a herniated disc to regress (would increase dehydration of the hernia, but this is controversial), or true arthritis to heal. Facet blocks of the mid-branch block type are not intended for therapy.
-
Symptomatic : In the majority of cases, the main goal is to reduce pain. Median branch block type facet blocks have an effect primarily on facet pain and referred segment pain. Intra-articular facet blocks add an effect on the root component.
A particular case of symptomatic effect is to facilitate the remusculation of a lumbar segment. Indeed, if a segment is "too painful", there is a protective reflex which prevents the muscles of this segment from working. In this case, it is illusory to want to strengthen this segment and whatever efforts are made, there will be no real resuscitation of the segment. One way to get around the problem is to make facet blocks on the affected segment, which will mask the pain and lift the segment's protective reflex. This will allow this segment to be built up on average for 3 to 4 months. -
Prognosis : Intra-articular facet blocks can give an idea of the reversibility of root damage. Indeed, if a nerve compression has become too chronic, part or all of the damage will become irreversible and the treatment of the cause of the compression will not lead to significant improvement.We often give an analogical example to the patient: "You buy a new pillow and put a large stone on it. If you remove the stone after 2 days, you will find a brand new pillow. If you remove the stone after 6 months, you will certainly no longer have it. compression, but the mark on the pillow will remain. ".
This lumbar MRI clearly illustrates the problem of segmental muscle atrophy. The musculature normally present (right image - dark gray) is replaced by fat (left image - light gray). These are images for two adjacent levels in the same patient.
In these situations, intra-articular facet blocks of the affected segment can significantly facilitate resuscitation of that segment.


This diagram illustrates the rationale for intra-articular facet injections for the treatment of herniated discs .
Benefits:
-
Diffusion of the drug close to both the hernia and the root
-
Prolonged effect because the intra-articular space is not vascularized
-
No risk of intrathecal or intravascular injection when using depot steroids
-
No volume effect in the spinal canal

Intra-articular lumbar facet blocks
Diagrams showing the intra-articular facet injection site for the lumbar spine.


This simplified diagram represents an axial lumbar section by illustrating the most important anatomical elements for facet blocks:
-
Nerve root
-
Yellow ligament
-
Cleft joint


Lumbar anatomy - Diagram of the dog:
The eye corresponds to the pedicle
The ear corresponds to the upper facet
The neck corresponds to the isthmus
The front leg corresponds to the lower facet
The hind leg corresponds to the spinous process
The body matches the blade

Lumbar facet blocks are the most common. They are performed in a room dedicated to the treatment of pain or in an operating theater. Our analgesia room meets the criteria for a level 1 operating room and is under positive pressure to reduce the risk of infection. All infiltrations are performed under sedation with the help of an anesthetist.
Technical:
Position : The patient is in the prone position ("prone"). We use a motorized operating table with a carbon plate as this allows better positioning of the patient without interfering with the location by fluoroscopy .
Preparation : The patient's back is disinfected extensively and draped similar to an operation for optimal sterility.
Spotting : The radioscopic spotting is now carried out with a Siemens Cios radioscopy with plane sensor which allows a better definition of the target by increasing the visualized area while reducing the geometric deformation. Fluoroscopy images are repeated on giant wall screens to avoid blind spots during procedures and improve operator visual comfort. A pulsed mode is used for radiation protection reasons.
Positioning of the fluoroscopy : The cleft joint is optimally visible with a coronal angle which varies according to the target level. This angle is about 30 degrees in L5-S1 to be practically zero in L1-L2. This angle is obtained by combining the angle of the fluoroscopy and the lateral tilt of the operating table (tilt). The sagittal angle can also be adapted according to the level and lumbar lordosis. These angles are not necessarily symmetrical between the left and the right!
Needle : A needle dedicated to this kind of application is used. It has several advantages: a short bevel, which limits the risk of leakage of the drug and untimely penetration of the bone or cartilage; a pipe connected without fitting with a very small lumen to limit the dead space and flexibility allowing easier guidance. We mainly use 2 lengths: 10 and 15 cm to adapt to the patient's morphology.



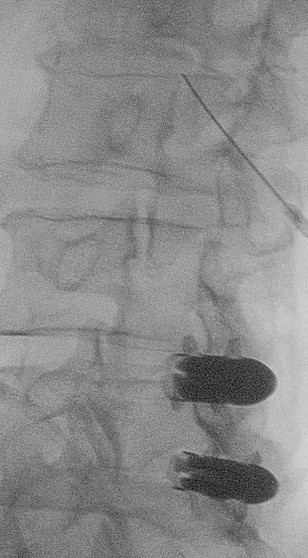
Left L4-L5 facet block : The left image clearly shows the L4-L5 articular cleft thanks to an oblique projection of approximately 30 degrees. The center image shows the needle in the cranial part of the L4-L5 cleft joint. The image on the right shows the L4-L5 arthrography with a fine cleft joint.



Right L3-L4 facet block : The image on the left clearly shows the L3-L4 joint cleft thanks to an oblique projection at approximately 30 degrees. The center image shows the needle in the cranial part of the L3-L4 cleft joint. The image on the right shows the L3-L4 arthrography with a very fine cleft joint .